BSC® Solutions
VOICES
Explore our FDA-focused solution areas to see how we support medical device and pharmaceutical companies across regulatory pathways and product types, from early strategy through approval-ready submissions.
BSC® Solutions
VOICES
Explore our FDA-focused solution areas to see how we support medical device and pharmaceutical companies across regulatory pathways and product types, from early strategy through approval-ready submissions.

Guidance Docs
Clinical Data Presentations for Orthopedic Device Applications
Published Dec 2, 2004
Guidance Docs
Clinical Data Presentations for Orthopedic Device Applications
Published Dec 2, 2004
Guidance Docs
Clinical Data Presentations for Orthopedic Device Applications
Published Dec 2, 2004
•
1 min read time
Clinical Data Presentations for Orthopedic Device Applications
What FDA Expects When You Present Clinical Data for an Orthopedic Device Submission
Most orthopedic device sponsors spend the bulk of their energy on study design, endpoint selection, and statistical analysis. By the time the submission is being assembled, clinical data presentation is treated as a formatting exercise — something the clinical writing team handles at the end. That's a mistake, and it's one we see regularly.
FDA has published specific guidance on how clinical data should be structured and presented for orthopedic device submissions — covering premarket approvals, investigational device exemption annual reports, premarket notifications, and post-approval study reports. The document is practical, detailed, and worth reading carefully. Here are the areas that matter most in practice.
Always Show the Denominator
The guidance makes this point directly in its opening recommendations: present data as "64/75 patients at 3 months" rather than "85% at the 3-month timepoint." The reason is straightforward. If 100 patients were enrolled but only 75 appear in your table, FDA wants to know what happened to the other 25. Reporting a rate without the denominator doesn't answer that question — it raises it.
This sounds basic, but it has real downstream consequences. Every table in your submission needs a clear statement of the population it's based on, and if that population is a subset of the enrolled cohort, you need to account for who's missing and why.
Patient Accounting Is a Formal Deliverable
FDA lays out a specific patient accounting framework that should appear in tabular form at every follow-up interval. The required elements are:
Theoretical follow-up is the number of patients who should have been evaluated at a given timepoint, determined by working backward from a pre-specified database closure date. For every enrolled patient, you calculate how much time elapsed between their implantation and database closure, and from that you determine which follow-up visits they should have attended. The sum across all patients at each scheduled visit is your theoretical follow-up.
Expected is theoretical follow-up minus cumulative deaths and failures at that interval. For certain statistical plans, patients "not yet overdue" — meaning they are within a follow-up window but haven't been evaluated yet — are also subtracted.
Actual refers specifically to patients with complete data for every safety and effectiveness endpoint required by the protocol, evaluated within the pre-specified time window. A patient who came in at the right time but is missing a radiograph, or whose pain score wasn't collected, does not count as "actual." This distinction matters — FDA also asks for an "all evaluated" row that captures patients with any data reviewed, even if incomplete.
Follow-up rate is simply Actual divided by Expected, expressed as a percentage.
That percentage has a specific threshold attached to it. For investigational device exemption and premarket approval submissions, FDA recommends a minimum of 85% follow-up in each study cohort. If a submission falls short of that, the agency expects a written explanation and a description of steps being taken to improve follow-up. Sensitivity analyses may also be required at final submission to justify pooling patients with incomplete or out-of-window data alongside those who were evaluated per protocol.
Follow-Up Windows Should Be Pre-Specified and Non-Overlapping
The guidance recommends defining evaluation windows before the study begins. The examples given are:
6 weeks ± 2 weeks
3 months ± 2 weeks
6 months ± 1 month
12 months ± 2 months
24 months ± 2 months
Annually ± 2 months
FDA's rationale is that pre-specified, non-overlapping windows produce more homogeneous patient groups at each timepoint, which makes comparisons across intervals more interpretable. When windows are continuous or undefined, it becomes ambiguous which visit belongs to which interval — and that ambiguity typically surfaces as a deficiency at submission rather than during study conduct, when it's far more expensive to address.
Adverse Events and Surgical Interventions Are Separate Presentations
FDA organizes safety into two distinct categories, and the guidance is explicit that they should be presented separately.
Adverse events — infections, wound complications, fractures, neurological events, systemic events — are presented in time-course tables with patient counts at each follow-up interval. The guidance recommends reporting all adverse events regardless of frequency. There is no threshold below which an event can be omitted.
Subsequent secondary surgical interventions get their own table with FDA-defined categories:
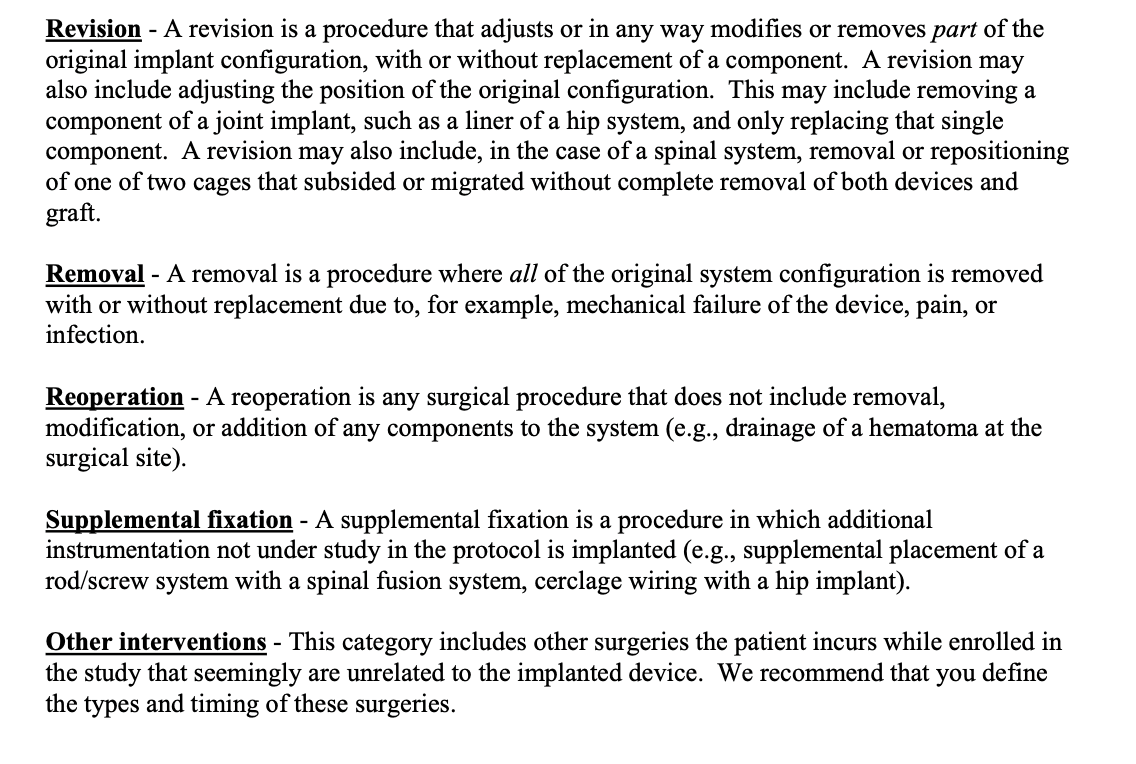
A revision involves changing part of the system; a removal involves taking out all of it. The guidance notes that not every removal automatically constitutes a failure — removing a pedicle screw system after confirmed fusion is different from removing a cage due to pseudoarthrosis. Sponsors need to pre-specify in their protocol which removals will be treated as failures and provide a rationale. If the protocol calls for planned removal of any component, how that will be interpreted in terms of study success or failure needs to be defined before enrollment begins.
The guidance also makes clear how to handle the timing of these events in the accounting table: a revision occurring between the immediate post-op visit and the three-month follow-up is reported at the three-month timepoint, not at the visit when it was discovered.
The Patient Success Table Requires More Than Effectiveness Parameters Alone
For spinal device studies, the FDA illustrates a patient success table that tracks, at each follow-up interval, the number of patients meeting each success criterion — fusion, Oswestry score improvement, neurological status, disc height, back pain, leg pain, and quality of life measures — along with an overall success row. For joint replacement studies, the same logic applies using the relevant scoring system, such as the Harris Hip Score.
This table requires that every component of your composite endpoint be tracked and documented for each patient at each visit. A patient who is missing one component — say, a radiograph required to assess fusion — cannot be classified as a success or failure on the composite endpoint for that timepoint. Of course, subjects who are known failures already can be treated as failures. This affects both the numerator and the denominator of your success rate, and consequently, whether your study achieves its pre-specified primary endpoint. It is a detail that gets missed frequently when data collection isn’t actively monitored against the endpoint structure throughout the study.
The Practical Implication
The standards described in this guidance document aren't formatting preferences. They reflect how FDA reviewers evaluate submissions, and departure from them — undefined follow-up windows, conflated adverse event categories, incomplete patient accounting, or missing endpoint components — generates deficiency letters. In our experience, the sponsors who move through review most efficiently are the ones who build these standards into their protocols and statistical analysis plans at the design stage, not the ones trying to reconstruct them during submission preparation.
If you're designing a spine or orthopedic trial, preparing an annual report, or approaching a premarket submission and want to make sure your clinical data presentation holds up under review, we're happy to talk through what that looks like for your specific device and study design.
Biomedical Statistical Consulting LLC (BSC®) has supported FDA regulatory submissions for orthopedic and spine device companies for nearly 40 years. Learn more at biomedstat.com.
References
https://www.fda.gov/media/71670/download

Let's help you find a path
to market
About BSC®
Working With BSC®
Services
Project logistics
Data and Software
What does BSC specialize in?
What types of clients do you work with?
What therapeutic areas do you cover?
How is BSC different from a CRO?
What size projects do you handle?
Let's help you find a path
to market
About BSC®
Working With BSC®
Services
Project logistics
Data and Software
What does BSC specialize in?
What types of clients do you work with?
What therapeutic areas do you cover?
How is BSC different from a CRO?
What size projects do you handle?
Let's help you find a path
to market
About BSC®
Working With BSC®
Services
Project logistics
Data and Software
What does BSC specialize in?
What types of clients do you work with?
What therapeutic areas do you cover?
How is BSC different from a CRO?
What size projects do you handle?
Let's help you find a path
to market
About BSC®
Working With BSC®
Services
Project logistics
Data and Software
What does BSC specialize in?
What types of clients do you work with?
What therapeutic areas do you cover?
How is BSC different from a CRO?
What size projects do you handle?
Featured Resources
Get regulatory insights
from BSC®



Featured Resources
Get regulatory insights
from BSC®
Featured Resources
Get regulatory insights
from BSC®
Featured Resources
Get regulatory insights
from BSC®
Request Expert Review
Backed by Regulatory Experience.
Engage directly with senior biostatisticians to review your clinical strategy, statistical approach, or FDA submission — with clarity, rigor, and regulatory perspective.
Confidential discussion with senior biostatisticians experienced in FDA submissions.
Request Expert Review
Backed by Regulatory Experience.
Engage directly with senior biostatisticians to review your clinical strategy, statistical approach, or FDA submission — with clarity, rigor, and regulatory perspective.
Confidential discussion with senior biostatisticians experienced in FDA submissions.
Request Expert Review
Backed by Regulatory Experience.
Engage directly with senior biostatisticians to review your clinical strategy, statistical approach, or FDA submission — with clarity, rigor, and regulatory perspective.
Confidential discussion with senior biostatisticians experienced in FDA submissions.
Request Expert Review
Backed by Regulatory Experience.
Engage directly with senior biostatisticians to review your clinical strategy, statistical approach, or FDA submission — with clarity, rigor, and regulatory perspective.
Confidential discussion with senior biostatisticians experienced in FDA submissions.
Use your preferred LLM to explore BSC®
Use your preferred LLM to explore BSC®